
Medizintourismus-Blog
Wirksame Behandlung der Adenomyose in Korea: Krämpfe mit modernen Verfahren lindern

Table of contents
- Was ist Adenomyose? Die Erkrankung verstehen
- Die Auswirkungen von Adenomyose-Krämpfen und Begleitsymptomen
- Häufige Bezeichnungen und Abgrenzung zu ähnlichen Erkrankungen
- Medizinische Verfahren bei Adenomyose: Ein umfassender Leitfaden
- Nichtoperative Ansätze: Symptomkontrolle mit Medikamenten und Hormontherapien
- Minimalinvasive und organerhaltende chirurgische Eingriffe: Erhalt der Gebärmutter
- Definitive chirurgische Behandlung: Hysterektomie
- Beste Kliniken in Korea bei Adenomyose-Krämpfen
- Ablauf und Kosten von Adenomyose-Behandlungen in Südkorea: Perspektive des Medizintourismus
- Patientenerfahrungen und Ergebnisse nach Adenomyose-Behandlungen
- Schlussfolgerungen
- Literaturverzeichnis
Planen Sie eine Behandlung in Korea? Alles, was Sie wissen müssen, z. B. wie Sie Betrug vermeiden, Visa, Dolmetscher und Tipps für die Erholung, finden Sie in unserem Master Guide für Medizintourismus. Planen Sie mit Vertrauen in Minuten statt in Wochen!
Dieser Bericht befasst sich ausführlich mit Adenomyose, einer gynäkologischen Erkrankung, von der viele Menschen betroffen sind. Er erklärt, was Adenomyose ist, beschreibt die Symptome, die Patientinnen erleben, und zeigt auf, wie sie sich von ähnlichen Erkrankungen unterscheidet. Dieses Verständnis hilft Patientinnen und medizinischen Fachkräften, fundierte Entscheidungen über Diagnostik und Behandlung zu treffen.
Was ist Adenomyose? Die Erkrankung verstehen
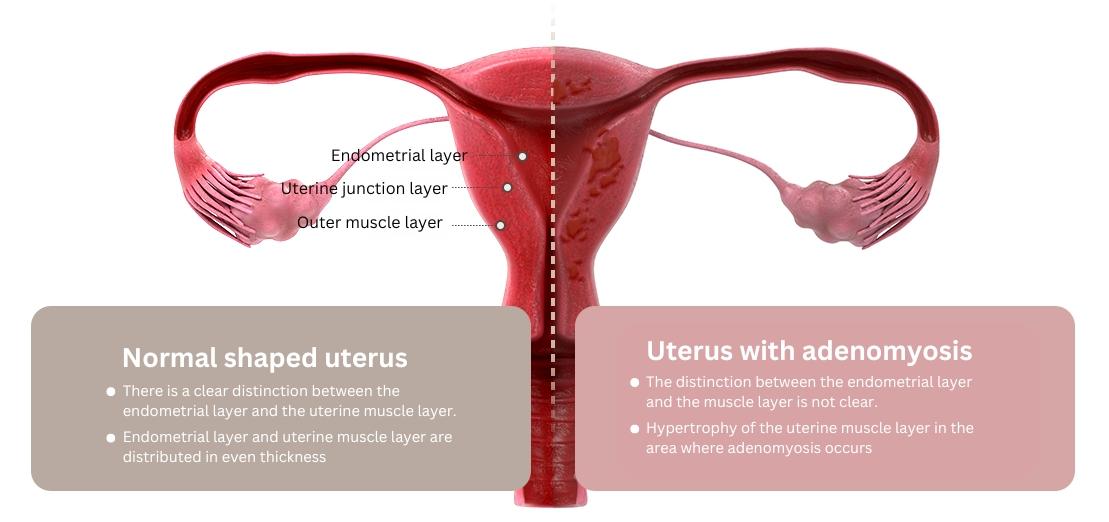
Adenomyose (ausgesprochen ad-en-o-my-O-sis) liegt vor, wenn Endometriumgewebe – also Gebärmutterschleimhaut – abnormal in die Muskelschicht der Gebärmutter, das sogenannte Myometrium, einwächst. Das unterscheidet sich von Endometriose, bei der ähnliches Gewebe außerhalb der Gebärmutter an Organen wie Eileitern, Eierstöcken, Vagina oder Darm wächst.
Das verlagerte Gewebe im Myometrium verdickt sich weiterhin, zerfällt und blutet während jedes Menstruationszyklus. Da dies jedoch innerhalb der Gebärmuttermuskulatur geschieht, vergrößert sich die Gebärmutter, und es kommt häufig zu schmerzhaften, starken Monatsblutungen. Adenomyose tritt in zwei Hauptformen auf: diffus, wenn sich das Gewebe über die gesamte Gebärmutterwand verteilt, und fokal, wenn es auf einen Bereich begrenzt ist, was mitunter als Adenomyom bezeichnet wird. Das Verteilungsmuster des Gewebes beeinflusst, welche Behandlungen am besten geeignet sind.
Die genaue Ursache der Adenomyose ist nicht vollständig geklärt. Zu den diskutierten Theorien zählen invasives Gewebewachstum, möglicherweise ausgelöst durch Gebärmutteroperationen wie Kaiserschnitte, eine Fehlplatzierung während der fetalen Entwicklung, Entzündungen nach der Geburt sowie die Beteiligung von Knochenmark-Stammzellen. Am häufigsten wird die Erkrankung bei Frauen in ihren 40ern und 50ern diagnostiziert. Zu den Risikofaktoren gehören Geburten sowie frühere Eingriffe an der Gebärmutter wie Kaiserschnitte, die Entfernung von Myomen oder eine Dilatation und Kürettage (D&C). Nach der Menopause bessern sich die Symptome in der Regel auf natürliche Weise, wenn die Menstruation ausbleibt.
Eine große Herausforderung besteht darin, dass die Symptome der Adenomyose denen anderer Erkrankungen wie Endometriose und Uterusmyomen stark ähneln. Diese Überschneidung kann die richtige Diagnose und Behandlung verzögern. Wenn Beschwerden anhalten oder Therapien nicht wirken, sind häufig weiterführende bildgebende Verfahren wie die Magnetresonanztomographie (MRT) erforderlich, um Adenomyose von anderen Ursachen abzugrenzen. Patientinnen sollten auf eine gründliche Abklärung bestehen und gegebenenfalls eine Zweitmeinung einholen, um eine möglichst genaue Diagnose zu erhalten.
Die Auswirkungen von Adenomyose-Krämpfen und Begleitsymptomen
Die starken Krämpfe, die durch Adenomyose verursacht werden, heißen medizinisch Dysmenorrhoe. Diese Krämpfe können stechend und sehr intensiv sein und den Alltag, die Arbeit, die Schule oder soziale Aktivitäten erheblich beeinträchtigen.
Neben Schmerzen verursacht Adenomyose häufig Menorrhagie, also starke oder verlängerte Monatsblutungen. Dies kann zu einer chronischen Anämie führen, die Müdigkeit, Schwindel, Ohnmachtsanfälle, Benommenheit und Kurzatmigkeit verursachen kann. Eine Anämie mindert die Lebensqualität und das Energieniveau oft deutlich.
Zu den weiteren Symptomen gehören chronische Beckenschmerzen außerhalb der Menstruation, Schmerzen beim Geschlechtsverkehr (Dyspareunie) sowie ein Gefühl von Blähung oder Schwere im Bauchraum. Die Gebärmutter kann vergrößert und druckschmerzhaft sein.
Adenomyose kann zudem die reproduktive Gesundheit beeinträchtigen, indem sie die Gebärmutterhöhle verformt, was die Einnistung eines Embryos stören und das Fehlgeburtsrisiko erhöhen kann. Sie ist mit einer erhöhten Wahrscheinlichkeit für Schwangerschaftskomplikationen wie hypertensive Erkrankungen, Schwangerschaftsdiabetes, postpartale Blutungen, vorzeitige Plazentalösung und Frühgeburt verbunden. Das Verständnis dieser weitreichenden Auswirkungen hilft Patientinnen, das volle Ausmaß der Adenomyose zu erkennen und eine umfassende Versorgung in Anspruch zu nehmen.
Häufige Bezeichnungen und Abgrenzung zu ähnlichen Erkrankungen
Starke Menstruationsschmerzen bei Adenomyose werden als Dysmenorrhoe bezeichnet, starke Blutungen als Menorrhagie. Manchmal wird Adenomyose fälschlicherweise als „innere Endometriose“ bezeichnet, weil beide Erkrankungen Endometriumgewebe betreffen.
Der entscheidende Unterschied liegt in der Lokalisation: Bei Adenomyose wächst Gewebe in die Gebärmuttermuskulatur (Myometrium) hinein, während bei Endometriose Gewebe außerhalb der Gebärmutter an anderen Organen wächst.
Trotz dieser Unterschiede haben Adenomyose, Endometriose und Uterusmyome viele gemeinsame Symptome wie starke Blutungen und Beckenschmerzen, und Adenomyose tritt häufig zusammen mit Myomen auf. Jede dieser Erkrankungen erfordert jedoch andere Behandlungsansätze.
Eine Fehldiagnose kann zu unwirksamen oder sogar schädlichen Behandlungen führen. So wird etwa die Endometriumablation, bei der die Gebärmutterschleimhaut zerstört wird, bei Adenomyose im Allgemeinen nicht empfohlen, weil sie das tiefer liegende Gewebe nicht erreicht und die Symptome verschlimmern kann. Patientinnen sollten auf einer präzisen Diagnose und einer spezialisierten Behandlung bestehen, anstatt sich mit einer allgemeinen Symptombehandlung zufriedenzugeben.
Tabelle 1: Häufige Symptome der Adenomyose und ihre Auswirkungen
| Symptom | Medizinischer Begriff | Beschreibung | Mögliche Auswirkungen |
|---|---|---|---|
| Starke Menstruationskrämpfe | Dysmenorrhoe | Stechender, messerartiger Beckenschmerz während der Menstruation, der den Alltag beeinträchtigt. | Beeinträchtigt Arbeit und Sozialleben; kann den Einsatz starker Schmerzmittel erforderlich machen; mindert die Lebensqualität. |
| Starke/verlängerte Perioden | Menorrhagie | Übermäßige Blutung, häufiger Wechsel von Binden/Tampons, Abgang von Blutgerinnseln. | Kann zu chronischer Anämie führen (Müdigkeit, Schwindel, Kurzatmigkeit); emotionale und alltagsbezogene Belastung. |
| Chronische Beckenschmerzen | Chronische Beckenschmerzen | Anhaltende Unterbauchschmerzen auch außerhalb der Menstruation. | Anhaltendes Unwohlsein, das tägliche Aktivitäten beeinträchtigt. |
| Schmerzen beim Geschlechtsverkehr | Dyspareunie | Schmerzen oder Beschwerden beim Geschlechtsverkehr. | Beeinträchtigt intime Beziehungen und das emotionale Wohlbefinden. |
| Bauchblähung/Schweregefühl | Völlegefühl/Druck im Bauch | Gefühl von Druck oder Blähung im Unterbauch. | Körperliches Unwohlsein und Druckschmerz. |
| Vergrößerte Gebärmutter | Vergrößerter Uterus | Gebärmutter größer als normal, manchmal tastbar. | Druckschmerz oder Druckgefühl im Unterbauch. |
| Fruchtbarkeitsprobleme | Unfruchtbarkeit/Fehlgeburtsrisiko | Schwierigkeiten, schwanger zu werden oder eine Schwangerschaft aufrechtzuerhalten; erhöhtes Fehlgeburtsrisiko. | Emotionale Belastung; Auswirkungen auf die Familienplanung. |
Medizinische Verfahren bei Adenomyose: Ein umfassender Leitfaden
Dieser Abschnitt behandelt die Behandlungsmöglichkeiten bei Adenomyose – von der nichtoperativen Symptomkontrolle bis hin zu definitiven Operationen – und erläutert die einzelnen Verfahren, die zu erwartenden Ergebnisse und wichtige Aspekte.
Nichtoperative Ansätze: Symptomkontrolle mit Medikamenten und Hormontherapien
Nichtoperative Behandlungen konzentrieren sich in erster Linie auf die Linderung der Symptome und heilen die Adenomyose nicht. Obwohl sie die Lebensqualität verbessern können, kehren die Symptome oft zurück, wenn die Behandlung beendet wird. Dieses Wissen hilft Patientinnen, realistische Erwartungen zu entwickeln und sich auf mögliche spätere Behandlungen vorzubereiten.
- Entzündungshemmende Medikamente (NSAR): Frei verkäufliche Medikamente wie Ibuprofen (Advil, Motrin IB) oder Naproxen verringern Menstruationsschmerzen und Entzündungen. Wenn sie ein bis zwei Tage vor Beginn der Menstruation eingenommen und während der Periode weitergeführt werden, können sie auch die Blutung reduzieren.
- Hormonpräparate: Diese regulieren den Menstruationszyklus und unterdrücken das abnorme Gewebewachstum.
- Kombinierte östrogen-progestinhaltige Verhütung (Pillen, Pflaster, Ringe): Reduziert starke Blutungen und Schmerzen; eine kontinuierliche Anwendung kann zum Ausbleiben der Menstruation (Amenorrhoe) führen und so Beschwerden lindern.
- Nur-Gestagen-Verhütung: Systeme wie die Mirena-Spirale geben Gestagen lokal ab, wodurch Krämpfe und Blutungen vermindert werden; häufig tritt dabei Amenorrhoe auf. Das Levonorgestrel-freisetzende Intrauterinsystem (LNG-IUS) kann die Lymphangiogenese reduzieren und so zur Symptomlinderung beitragen.
- Gonadotropin-Releasing-Hormon-(GnRH)-Agonisten: Versetzen den Körper durch die Senkung des Östrogenspiegels vorübergehend in einen menopauseähnlichen Zustand und lindern dadurch Symptome. Wegen ihrer Nebenwirkungen werden sie meist nur bei ausgewählten Patientinnen und für kurze Zeit eingesetzt.
- Tranexamsäure: Ein nicht hormonelles Medikament, das an Tagen mit starker Blutung eingenommen wird, um die Blutung zu verringern.
- Weitere unterstützende Maßnahmen: Warme Bäder, Wärmekissen, entzündungshemmende Ernährung und Beckenbodenphysiotherapie können helfen, Schmerzen zu kontrollieren und die Funktion der Beckenmuskulatur zu verbessern.
Minimalinvasive und organerhaltende chirurgische Eingriffe: Erhalt der Gebärmutter
Diese Optionen eignen sich besonders für Patientinnen, die ihre Gebärmutter erhalten möchten, insbesondere wenn sie sich Kinder wünschen. Bei der Wahl dieser Behandlungen müssen Kinderwunsch, Invasivität und Risiken sorgfältig gegeneinander abgewogen werden.
-
Uterusarterienembolisation (UAE):
- Beschreibung: Ein nichtoperatives, bildgesteuertes Verfahren, das von einer interventionellen Radiologin oder einem interventionellen Radiologen unter örtlicher Betäubung durchgeführt wird. Ein Katheter wird in eine Arterie (in der Leiste oder am Handgelenk) eingeführt und bis zu den Gebärmutterarterien vorgeschoben. Winzige Partikel blockieren die Blutzufuhr zu Adenomyoseherden, sodass diese schrumpfen, während gesundes Gewebe geschont wird.
- Ablauf: Nach örtlicher Betäubung wird ein Katheter eingeführt und mithilfe von Röntgen und Kontrastmittel verfolgt. Embolisations-Mikroperlen werden injiziert, um die Blutversorgung zu blockieren. Anschließend wird der Katheter entfernt und ein Druckverband angelegt. Der Eingriff dauert 45–90 Minuten und ist in der Regel währenddessen schmerzfrei.
- Erholung: Der Krankenhausaufenthalt beträgt meist 24–48 Stunden, manchmal ist auch eine ambulante Durchführung möglich. Leichte bis mäßige Krämpfe und Müdigkeit halten einige Tage bis etwa eine Woche an. Leichte Aktivitäten sind nach 3–5 Tagen wieder möglich; die vollständige Erholung dauert 1–2 Wochen und ist damit schneller als nach einer Hysterektomie.
- Ergebnisse: 75–83,1 % der Patientinnen berichten über eine Symptomverbesserung; im MRT zeigt sich eine Verkleinerung der Gebärmutter. Etwa 88–90 % sind mit der langfristigen Linderung von Schmerzen, Blutungen und Druckbeschwerden zufrieden. Eine Studie zeigte, dass 82 % über 7 Jahre hinweg eine Hysterektomie vermeiden konnten.
- Vorteile: Minimalinvasiv, keine Vollnarkose, keine Nähte, geringer Blutverlust, keine größeren Narben, Erhalt der Gebärmutter, schnellere Erholung.
- Risiken/Nebenwirkungen: Geringes Komplikationsrisiko; möglich sind Gefäßverletzungen, Blutungen, Blutergüsse an der Einstichstelle, allergische Reaktionen auf Kontrastmittel sowie ein vorübergehendes Postembolisationssyndrom (Fieber, Unwohlsein für 5–7 Tage).
-
Adenomyomektomie:
- Beschreibung: Chirurgische Entfernung von adenomyotischem Gewebe unter Erhalt der Gebärmutter, ähnlich der Entfernung von Myomen (Myomektomie). Am besten geeignet bei fokaler Adenomyose.
- Ablauf: Die Herde werden sorgfältig über eine laparoskopisch assistierte Mini-Laparotomie oder eine offene Operation entfernt. Die Gebärmutterwand wird mit Techniken wie der Doppel- oder Dreifach-Lappenmethode rekonstruiert, um Rückfälle zu verringern.
- Ergebnisse: Etwa 75 % erleben eine Linderung starker Krämpfe und starker Blutungen. Die Schwangerschaftsergebnisse variieren: Eine Studie zeigte 30 % klinische Schwangerschaften und 16 % Lebendgeburten; eine andere berichtete über 41,9 % Schwangerschaften und 29 % Lebendgeburten.
- Risiken/Einschränkungen: Aufgrund des infiltrativen Charakters ist eine vollständige Entfernung schwierig; die Rezidivrate liegt zwischen 22 und 72 %. Schwangerschaften nach der Operation gehen mit einem erhöhten Risiko für eine Uterusruptur einher. Es können Verwachsungen entstehen. Eine laparoskopische Entfernung kann unvollständig sein.
-
Endometriumablation:
- Beschreibung: Hierbei wird mit Hitze die Gebärmutterschleimhaut zerstört.
- Ergebnisse/Einschränkungen: Kann starke Blutungen verringern, wird bei Adenomyose jedoch im Allgemeinen nicht empfohlen, weil das tiefer liegende Gewebe nicht behandelt wird und sich Schmerzen verschlimmern können. Geeignet nur für Frauen mit abgeschlossener Familienplanung.
Die Wahl der Behandlung hängt von persönlichen Faktoren ab, etwa vom Kinderwunsch, von der Bereitschaft zu einem operativen Eingriff und von der Akzeptanz eines Rückfallrisikos. Die Hysterektomie ist die einzige heilende Behandlung, doch viele bevorzugen den Erhalt der Gebärmutter. Die UAE bietet ein gutes Gleichgewicht aus Symptomlinderung, geringer Invasivität und schneller Erholung. Die Adenomyomektomie kann die Fruchtbarkeit erhalten, ist jedoch mit höheren Risiken verbunden. Von der Endometriumablation wird meist abgeraten. Patientinnen sollten die Optionen ausführlich mit spezialisierten Fachärztinnen und Fachärzten besprechen, damit die Behandlung ihren Prioritäten entspricht.
Definitive chirurgische Behandlung: Hysterektomie
- Beschreibung: Die chirurgische Entfernung der Gebärmutter; sie gilt als „Goldstandard“ und einzige sichere Heilung der Adenomyose.
- Operationsarten: Kann abdominal (großer Schnitt), laparoskopisch (kleine Schnitte) oder vaginal (über die Scheide) durchgeführt werden. Die Wahl hängt von der Größe der Gebärmutter, dem Gesundheitszustand und der Erfahrung der Operateurin oder des Operateurs ab.
- Erhalt der Eierstöcke: In der Regel werden die Eierstöcke belassen, um die Hormonproduktion aufrechtzuerhalten, da sich Adenomyose nach der Menopause zurückbildet.
- Ergebnisse: Entfernt das adenomyotische Gewebe vollständig und beseitigt starke Blutungen. Viele Patientinnen berichten über eine deutliche Linderung von Schmerzen, Blähungen und Unwohlsein und darüber, ihr Leben mit mehr Wohlbefinden, besser sitzender Kleidung und mehr Energie zurückgewonnen zu haben.
- Zu beachten: Größere Operation mit längerer Erholungszeit (3–6 Wochen bei abdominalem Vorgehen; kürzer bei laparoskopischen/robotischen Verfahren). Eine dauerhafte Lösung, die bei schweren, auf andere Behandlungen nicht ansprechenden Symptomen sowie bei fehlendem Kinderwunsch empfohlen wird. Manche Patientinnen stoßen auf Widerstand seitens Behandelnder oder der Familie, besonders wenn sie kinderlos sind.
- Einschränkungen: Obwohl die Erkrankung entfernt wird, kann die Schmerzlinderung unvollständig sein, insbesondere bei Patientinnen mit chronischen Schmerzen oder vorherigem Opioidgebrauch. Eine präoperative Beratung sollte realistische Erwartungen vermitteln und ein fortlaufendes Schmerzmanagement thematisieren.
Tabelle 2: Behandlungsoptionen bei Adenomyose: Ein vergleichender Überblick
| Behandlungskategorie | Konkretes Verfahren | Primäres Ziel | Invasivität | Erhalt der Gebärmutter | Erholungszeit | Zentrale Ergebnisse | Zu beachten/Einschränkungen |
|---|---|---|---|---|---|---|---|
| Nichtoperativ | NSAR (z. B. Ibuprofen) | Symptomkontrolle (Schmerzen, Blutung) | Nichtinvasiv | Ja | Minimal | Verringerung von Schmerzen und Blutung während der Periode | Heilt nicht; Symptome können zurückkehren; zeitlich begrenzte Wirksamkeit |
| Hormontherapie (Pillen, IUPs, GnRH-Agonisten) | Symptomkontrolle (Blutung, Schmerzen) | Nichtinvasiv | Ja | Minimal | Reguliert den Zyklus, reduziert Blutung/Schmerzen, kann Amenorrhoe auslösen | Heilt nicht; Symptome können zurückkehren; GnRH-Agonisten haben Nebenwirkungen | |
| Tranexamsäure | Symptomkontrolle (starke Blutung) | Nichtinvasiv | Ja | Minimal | Verringert den menstruellen Blutverlust | Nicht hormonell; Einnahme an Tagen mit starker Blutung | |
| Minimalinvasive/organerhaltende Chirurgie | Uterusarterienembolisation (UAE) | Schrumpfung adenomyotischen Gewebes, Symptomreduktion | Minimalinvasiv (Katheter) | Ja | 1–2 Wochen | 75–83,1 % Symptomverbesserung; kleinere Gebärmutter; hohe Zufriedenheit | Leichte Schmerzen/Müdigkeit nach dem Eingriff; mögliches Postembolisationssyndrom; Adenomyose wird unter Umständen nicht vollständig beseitigt |
| Adenomyomektomie | Entfernung adenomyotischen Gewebes, Erhalt der Gebärmutter | Chirurgisch (laparoskopisch/offen) | Ja | Variabel | Symptomlinderung; Erhalt der Fruchtbarkeit möglich | Hohe Rezidivrate (22–72 %); Risiko einer Uterusruptur in der Schwangerschaft; vollständige Entfernung schwierig | |
| Endometriumablation | Verringerung starker Blutungen | Minimalinvasiv (Hitze) | Ja | Kurz | Verringerte Blutung | Behandelt kein tiefes Gewebe; bei Adenomyose nicht empfohlen; kann Schmerzen verschlimmern; nur bei abgeschlossener Familienplanung | |
| Definitive Chirurgie | Hysterektomie | Vollständige Heilung der Adenomyose | Chirurgisch (abdominal/laparoskopisch/vaginal) | Nein | 3–6 Wochen (abdominal); kürzer laparoskopisch/robotisch | Vollständige Beseitigung der Erkrankung; behebt starke Blutungen; deutliche Schmerzlinderung bei vielen | Größere Operation; dauerhaft; längere Erholung; Schmerzreduktion kann variieren; realistische Erwartungen erforderlich |
Beste Kliniken in Korea bei Adenomyose-Krämpfen
Nachfolgend sind die besten Kliniken in Korea bei Adenomyose-Krämpfen aufgeführt:
| Klinikname | Hauptmerkmale | Besondere Techniken |
|---|---|---|
| SH Clinic | - Führendes multidisziplinäres Zentrum in Sinsa, Seoul - Ausschließlich auf Frauen ausgerichtete Klinik mit Fokus auf Komfort, Privatsphäre und Frauengesundheit - Alle gynäkologischen Operationen werden von einer preisgekrönten, fachärztlich zertifizierten Gynäkologin durchgeführt - Für exzellente Versorgung vom koreanischen Ministerium für Gesundheit und Wohlfahrt ausgezeichnet - Integrierter Zugang zu Hormonanalysen, Beckenboden-Therapie sowie ästhetischen oder rekonstruktiven Eingriffen - Hochmoderne, patientenorientierte Einrichtung | - Fortschrittliche regenerative Therapien, einschließlich Stammzellbehandlungen - Minimalinvasive Optionen - Personalisierte und umfassende Versorgung bei Adenomyose-Krämpfen |
| Cheongdam HIFU Clinic | - Führendes gynäkologisches Zentrum mit Spezialisierung auf Erkrankungen der Gebärmutter und Eierstöcke - One-Stop-Klinik für Diagnose und Behandlung - Fokus auf gebärmuttererhaltende Therapien - Hochqualifiziertes Team und modernste Technologie - Spezialisierte Zentren für Eierstockzysten- und Endometriose-Sklerotherapie | - Behandlung der Adenomyose mit hochintensiv fokussiertem Ultraschall (HIFU) - Minimalinvasive laparoskopische und Da-Vinci-roboterassistierte Operationen - Hysteroskopische intrauterine Eingriffe - Nichtoperative Sklerotherapie bei gynäkologischen Erkrankungen |
SH Clinic
Die SH Clinic in Sinsa, Seoul, ist ein führendes multidisziplinäres medizinisches Zentrum, das für seinen modernen Ansatz in der Stammzelltherapie, gynäkologischen Versorgung, ästhetischen Dermatologie und modernen plastischen Chirurgie bekannt ist. Als spezialisierte Frauenklinik zeichnet sich die SH Clinic durch personalisierte und umfassende Behandlungen in einer angenehmen, auf Frauen ausgerichteten Umgebung aus. Alle chirurgischen Eingriffe und gynäkologischen Behandlungen werden direkt von einer sehr erfahrenen, fachärztlich zertifizierten Gynäkologin durchgeführt, die mit einer offiziellen Auszeichnung des koreanischen Ministers für Gesundheit und Wohlfahrt geehrt wurde. Dieses außergewöhnlich hohe Maß an Expertise gewährleistet größtmögliche Sicherheit, Präzision und patientenorientierte Betreuung, insbesondere für Frauen mit belastenden Erkrankungen wie Adenomyose-Krämpfen.
Wichtige Gründe, warum die SH Clinic eine gute Wahl zur Behandlung von Adenomyose-Krämpfen ist:
- Ausschließlich auf Frauen spezialisierte Klinik, konzipiert für Komfort, Privatsphäre und Sensibilität für frauenspezifische Gesundheitsanliegen.
- Alle gynäkologischen Operationen und Eingriffe werden von einer preisgekrönten, fachärztlich zertifizierten Gynäkologin durchgeführt.
- Umfassender Ansatz mit konventionellen und fortschrittlichen regenerativen Therapien, einschließlich Stammzellbehandlungen und minimalinvasiven Optionen.
- Sorgfältige und einfühlsame Betreuung vor und nach dem Eingriff, abgestimmt auf die individuellen Bedürfnisse jeder Patientin.
- Integrierter Zugang zu verwandten Spezialgebieten wie Hormonanalysen, Beckenboden-Therapie sowie ästhetischer oder rekonstruktiver gynäkologischer Chirurgie.
- Vom koreanischen Ministerium für Gesundheit und Wohlfahrt für Exzellenz in der Frauengesundheit ausgezeichnet.
- Hochmoderne Einrichtung, die neueste Technologie mit patientenorientierten, ganzheitlichen Behandlungskonzepten verbindet.
Für alle, die in Korea unter Adenomyose-Krämpfen oder verwandten gynäkologischen Beschwerden leiden, bietet die SH Clinic eine Möglichkeit zur nachhaltigen Linderung und einen Weg zu mehr Wohlbefinden.
Ihre Website finden Sie hier: SH Clinic Website
Cheongdam HIFU Clinic
Die Cheongdam HIFU Clinic ist ein führendes gynäkologisches Zentrum in Korea, das sich der umfassenden Versorgung von Frauen widmet, die an Erkrankungen wie Adenomyose und den damit verbundenen Krämpfen leiden. Als One-Stop-Klinik ist Cheongdam sowohl auf die Diagnose als auch auf die Behandlung von Gebärmutter- und Eierstockserkrankungen spezialisiert und bietet ein breites Spektrum medizinischer Lösungen – von nichtoperativen Interventionen bis hin zu fortgeschrittenen chirurgischen Verfahren. Das herausragende Angebot der Klinik ist die Behandlung mit hochintensiv fokussiertem Ultraschall (HIFU), die besonders wirksam bei der Verkleinerung adenomyotischer Herde und der Linderung von Symptomen wie Beckenschmerzen und starken Monatsblutungen ist – und damit eine attraktive Option für Frauen darstellt, die eine gebärmuttererhaltende Therapie wünschen.
Neben HIFU zeichnet sich die Cheongdam HIFU Clinic durch minimalinvasive und fortschrittliche chirurgische Verfahren aus, darunter laparoskopische und Da-Vinci-roboterassistierte Operationen sowie hysteroskopische Techniken für intrauterine Erkrankungen. Diese hochmodernen Methoden ermöglichen eine schnellere Erholung, minimale Narbenbildung und eine höhere chirurgische Präzision. Die Klinik verfügt außerdem über spezialisierte Zentren für die Sklerotherapie bei Eierstockzysten und Endometriose und stellt damit auch nichtoperative Behandlungsoptionen für komplexe gynäkologische Erkrankungen bereit. Mit einem hochqualifizierten medizinischen Team und modernster Technologie bietet die Cheongdam HIFU Clinic individuelle und hochwertige Versorgung für Frauen, die unter den belastenden Auswirkungen von Adenomyose und Menstruationskrämpfen leiden.
Mehr über diese Klinik erfahren Sie hier: Cheongdam HIFU Clinic Website
Ablauf und Kosten von Adenomyose-Behandlungen in Südkorea: Perspektive des Medizintourismus
Südkorea ist ein führendes Ziel für Medizintourismus, insbesondere für fortschrittliche gynäkologische Versorgung, dank moderner Einrichtungen, erfahrener Ärztinnen und Ärzte sowie wettbewerbsfähiger Preise.
Ablauf einer Behandlung in Südkorea
Internationale Patientinnen durchlaufen in der Regel die folgenden Schritte:
- Erstberatung und Planung: Patientinnen besprechen ihren Zustand mit Ärztinnen und Ärzten und erörtern die Behandlungsoptionen. Hilfreich ist es, frühere Befunde wie Blutuntersuchungen, Ultraschall oder MRT mitzubringen.
- Voruntersuchungen: Untersuchungen wie Ultraschall und allgemeine Gesundheitschecks sind eingeschlossen, um die Eignung für den Eingriff sicherzustellen. Einige Pakete beinhalten Tests der ovariellen Reserve (AMH). Vor einer Operation wird ein Anästhesiegespräch angesetzt.
- Finanzielle Regelungen: In der Regel ist eine Anzahlung von 10 % erforderlich. Krankenhäuser stellen im Voraus Kostenvoranschläge zur Verfügung.
- Krankenhausaufenthalt und Betreuung: Die Kosten decken den Krankenhausaufenthalt ab (bei Operationen wie Myomektomie oft etwa 4 Tage), einschließlich Mahlzeiten und Überwachung der Erholung.
- Nachsorge: Die Nachsorge dient dazu, den Behandlungserfolg sicherzustellen und mögliche Probleme frühzeitig zu erkennen.
- Komfort- und Serviceleistungen: Viele Krankenhäuser bieten Einzelzimmer, Flughafentransfers und Dolmetscherdienste an, um Kommunikation und Komfort zu verbessern.
- Visum- und Einreisebestimmungen: Staatsangehörige aus 96 Ländern können für 30–180 Tage visumfrei einreisen. COVID-19-Tests und das Tragen von Masken in Kliniken können erforderlich sein.
Kosten von Adenomyose-Behandlungen in Südkorea und internationaler Vergleich
Die Kosten variieren je nach Verfahren, Komplexität der Erkrankung und Einrichtung, doch im Allgemeinen bietet Südkorea niedrigere Preise als Nordamerika oder Europa.
- Allgemeine Behandlung der Adenomyose: 1.500 bis 7.500 USD (₩2.180.000 - ₩10.900.000 KRW).
- Spezifische Verfahren:
- Beratung und Planung: ~25 USD (₩36.000 KRW).
- Uterusarterienembolisation (UAE): ₩3.000.000–₩7.000.000 KRW (~2.076 - 4.844 USD). Manche Quellen nennen für eine Myomektomie Preise ab 6.700 USD.
- Hysterektomie: 4.230 bis 21.000 USD (₩6.113.580 - ₩30.346.110 KRW). Standard: 5.000–15.000 USD; laparoskopisch ~6.770 USD; robotisch 12.000–20.000 USD.
- Adenomyomektomie: Nicht ausdrücklich aufgeführt, aber Myomektomie liegt zwischen 471 und 10.920 USD (₩684.000 - ₩15.875.000 KRW), vermutlich in einem ähnlichen Bereich.
- Diagnostik: Ultraschall ~25 USD; Becken-CT ~74 USD; MRT-Befundrevision ~15 USD.
- Internationaler Kostenvergleich:
- Behandlung der Adenomyose insgesamt:
- Südkorea: 1.500 - 7.500 USD
- USA: 500 - 5.000 USD (allgemein), 28.200 USD insgesamt
- Mexiko: 1.600 - 2.000 USD (endometriosebezogen)
- Türkei: 3.500 - 4.000 USD (Operation)
- Thailand: 4.500 - 5.000 USD (fokale Adenomyose günstiger als in den USA/Europa)
- Indien: 5.500 - 6.200 USD
- Kolumbien: 11.700 USD
- Australien: MRT bis zu 275 USD
- Hysterektomie:
- Südkorea: 4.230 - 21.000 USD
- USA: 4.217 - 20.000 USD (laparoskopisch bis zu 49.526 USD)
- Mexiko: 2.000 - 5.500 USD
- Türkei: 2.500 - 8.000 USD
- Thailand: 2.269 - 12.440 USD
- Australien: 8.000 - 15.000 USD
- Behandlung der Adenomyose insgesamt:
Südkorea bietet eine kosteneffiziente Option mit hochwertiger Versorgung und umfassenden Paketen, die Krankenhausaufenthalt, Beratungen und Unterstützungsleistungen einschließen. Reise- und Unterkunftskosten sollten bei der Planung des Medizintourismus zusätzlich berücksichtigt werden.
Patientenerfahrungen und Ergebnisse nach Adenomyose-Behandlungen
Patientinnen berichten nach der Behandlung häufig über eine deutliche Symptomlinderung, wobei die Erfahrungen je nach Verfahren unterschiedlich ausfallen.
- Uterusarterienembolisation (UAE): Viele beschreiben eine deutliche Besserung mit leichteren, kürzeren Perioden und minimalen Schmerzen. Die Erholung verläuft schneller als nach einer Hysterektomie, und viele nehmen innerhalb einer Woche ihre normalen Aktivitäten wieder auf. Patientinnen fühlen sich „großartig“ und sicherer, ohne die Sorge vor starken Blutungen und Schmerzen. Das Verfahren ist unkompliziert, wird unter örtlicher Betäubung durchgeführt, und die Schmerzen nach dem Eingriff sind meist gut beherrschbar. Auch wenn es keine vollständige Heilung ist, bietet die UAE den meisten eine langfristige Symptomlinderung.
- Adenomyomektomie: Patientinnen berichten über eine sofortige Linderung von Symptomen wie Ischiasschmerzen sowie weniger Blutungen und Beckenschmerzen. Manche benötigen keine Schmerzmittel mehr. Die Erholung kann langsamer verlaufen, insbesondere wenn der Eingriff mit anderen Operationen kombiniert wird. Die Linderung kann 3–5 Jahre anhalten, Rückfälle sind jedoch möglich. Für viele bestätigt der pathologische Nachweis von Adenomyose und Endometriose die Ursache jahrelang unerkannt gebliebener Schmerzen.
- Hysterektomie: Sie gilt als definitive Heilung, und viele Patientinnen erleben eine lebensverändernde Linderung von Schmerzen, Blähungen und Unwohlsein. Sie berichten oft, ihr Leben zurückgewonnen zu haben – mit mehr Komfort, besser sitzender Kleidung und mehr Energie. Die Erholung variiert je nach Operationsmethode. Patientinnen schätzen die Freiheit von periodenbezogenen Sorgen, was Selbstvertrauen und Beziehungen verbessern kann. Manche benötigen jedoch weiterhin Schmerzmanagement, wenn bereits vor der Operation chronische Schmerzen bestanden.
Schlussfolgerungen
Adenomyose verursacht starke Menstruationsschmerzen (Dysmenorrhoe), starke Blutungen (Menorrhagie), chronische Beckenschmerzen und Fruchtbarkeitsprobleme, da Endometriumgewebe in die Gebärmuttermuskulatur einwächst. Ihre Symptome überschneiden sich mit denen von Endometriose und Myomen, weshalb eine genaue Diagnose entscheidend ist.
Die Behandlungen reichen von der Symptomkontrolle mit NSAR und Hormonen bis hin zu operativen Verfahren. Nichtoperative Therapien lindern die Symptome, heilen die Adenomyose jedoch nicht und haben möglicherweise nur eine begrenzte Wirkdauer. Die Uterusarterienembolisation bietet wirksame Symptomlinderung bei Erhalt der Gebärmutter und schneller Erholung. Die Adenomyomektomie kann die Fruchtbarkeit erhalten, geht jedoch mit Risiken wie Rückfällen und Uterusruptur einher. Die Endometriumablation wird im Allgemeinen nicht empfohlen. Die Hysterektomie ist die einzige definitive Heilung, beseitigt die Erkrankung und starke Blutungen, wobei die Schmerzlinderung unterschiedlich ausfallen kann.
Südkorea bietet fortschrittliche und bezahlbare Versorgung bei Adenomyose mit umfassenden Leistungen für internationale Patientinnen und ist damit ein attraktives Ziel für Medizintourismus.
Die richtige Behandlung hängt von der Schwere der Symptome, dem Kinderwunsch und den persönlichen Vorlieben ab. Patientinnen sollten ihre Optionen ausführlich mit medizinischen Fachkräften besprechen, um die beste Lösung für ihre Gesundheitsziele und ihren Lebensstil zu finden.
Literaturverzeichnis
1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50
Häufig gestellte Fragen
Verwandte Blogbeiträge

Clitoroplasty in Korea: Methods, Candidacy, Recovery, Risks and Travel Planning
Aktualisiert: Aug 5, 2026

Bei vaginaler Trockenheit: PRP zur Vaginalverjüngung, Vaginalfiller und Stammzellbehandlungen zur Verbesserung der Sexualfunktion in Korea
Vaginale Trockenheit ist eine häufige Beschwerde, die durch unzureichende Lubrikation und Veränderungen der Gesundheit des Vaginalgewebes gekennzeichnet ist. Sie kann Schmerzen beim Sitzen, bei körperlicher Aktivität, beim Wasserlassen und beim Geschlechtsverkehr (Dyspareunie) verursachen und das sexuelle Verlangen sowie die Orgasmusfähigkeit beeinträchtigen. Die Folgen sind sowohl körperlich als
Aktualisiert: Jun 30, 2026

Vorehelicher Check-up zur pränatalen Gesundheitsvorsorge in Korea
Die Familienplanung ist ein bedeutender Meilenstein, der weit über den Hochzeitstag hinausgeht. Sie umfasst proaktive Schritte, um sicherzustellen, dass beide Partner gesund sind und eine stabile Grundlage für ihre zukünftigen Kinder schaffen können. Angesichts der Fülle an Gesundheitsinformationen im Internet ist es wichtiger denn je, bei komplexen Themen wie dem „prenatal health screening“ auf v
Aktualisiert: Jun 29, 2026
Pre-Marriage STI Testing in Korea: Benefits of Premarital Check-up for Safe Children
Aktualisiert: Jun 26, 2026

