Medical Tourism Blog
Dry Eye causes - Samsung Miracle Eye
Table of contents
- Introduction: Why Dry Eye Feels So Confusing
- What Actually Causes Dry Eye Syndrome?
- The Cost and Insurance Question: What Patients Are Worried About
- Dry Eye After Surgery: Why Cataract Patients Often Feel It More
- How I Decide Treatment: Severity First, Then Step-by-Step
- Artificial Tears: The Foundation (and When They’re Not Enough)
- Evaporative Dry Eye and Meibomian Gland Dysfunction: Warm Compresses and IPL
- Aqueous-Deficient Dry Eye and Sjögren’s: Keeping Tears on the Eye Longer
- When Dry Eye Becomes Severe: Protecting the Cornea
- Conclusion: A Practical Way to Think About Dry Eye
- More about Samsung Miracle Eye Clinic
Considering treatment in Korea? Everything you need to know e.g. — how to avoid scams, visas, interpreters, recovery tips — in our Medical Tourism Master Guide. Plan with confidence in minutes, not weeks!
Disclaimer: The following is a guest post. The information and opinions expressed are not of koreaclinicguide.com but of Samsung Miracle Eye Clinic
Introduction: Why Dry Eye Feels So Confusing
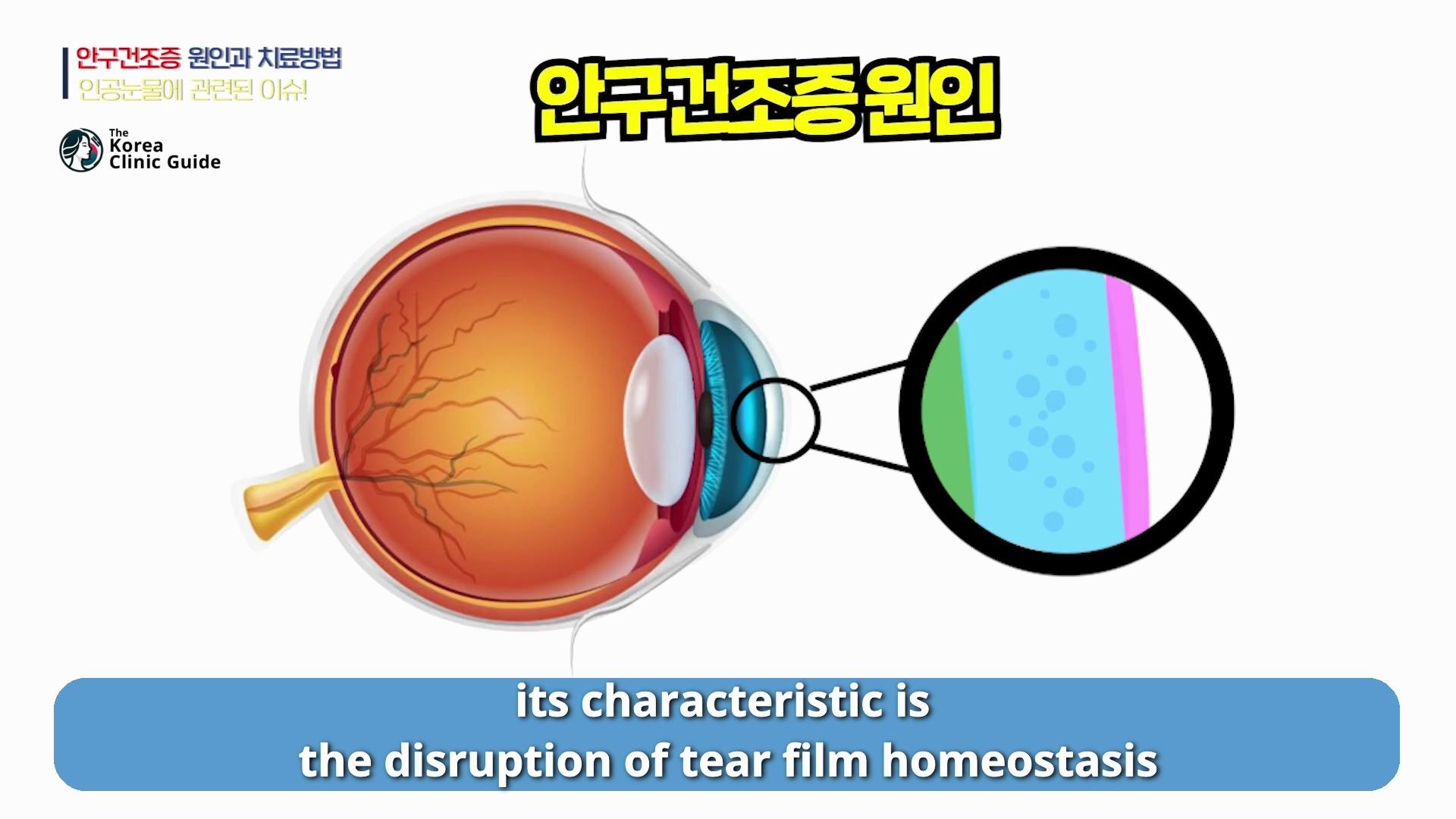
Dry eye is one of those conditions that sounds simple—“my eyes feel dry”—but in real life it’s rarely caused by just one thing. In the most authoritative definitions of dry eye syndrome, the key feature is a disruption in tear film homeostasis, meaning the tear film is no longer stable and balanced the way it should be. That instability can be triggered by many different factors, and in clinic I often see those causes overlapping rather than appearing neatly separated.
Because the causes blend together, I don’t decide treatment based on a single label alone. I decide how aggressively to treat based on symptom severity and how much the dryness is affecting daily life. Some people do well with habit changes and basic drops. Others need step-by-step escalation, procedures, or specialized care.
What Actually Causes Dry Eye Syndrome?
When I explain dry eye, I start with the tear film. A healthy tear film is not “just water.” It has multiple layers and functions: it lubricates, protects the ocular surface, supports clear vision, and keeps the eye comfortable. Dry eye syndrome develops when that tear film balance breaks down.
In practice, many patients ask, “So what is my cause?” The honest answer is that the causes are not always clearly distinct. For example, a patient may have increased tear evaporation from Meibomian gland dysfunction, while also having lifestyle triggers such as long hours on a smartphone, plus age-related changes that reduce baseline tear stability. These don’t just add up—they interact, which is why symptoms can fluctuate from day to day.
This is also why severity matters so much. Since different mechanisms can overlap, treatment isn’t a one-size-fits-all recipe. It’s a stepwise plan guided by how the eye is behaving and how uncomfortable the patient feels.
The Cost and Insurance Question: What Patients Are Worried About
A very common concern I hear is: “If my condition is classified as dry eye syndrome and insurance benefits don’t apply, making out-of-pocket costs high, what should I do?” That anxiety is understandable, especially when dry eye becomes a long-term issue.
To be realistic, even now, after vision correction surgery, the first three months typically involve artificial tears, antibiotics, and anti-inflammatory eye drops—and these are not covered by insurance. So for many post-operative patients, some degree of out-of-pocket cost is already part of the recovery process.
When it comes to how big a difference insurance changes might make, the impact depends on your situation. For procedures like SMILE or lens implant surgery, which we primarily perform, the effect on dry eye tends to be smaller, and the period of intensive artificial tear use typically doesn’t exceed about three months. In that setting, compared with the current post-operative routine, the “felt difference” for many patients may not be dramatic.
However, with LASIK or LASEK, the recovery period is longer, so the burden can be greater. And a bigger impact is often felt by patients undergoing intraocular surgery, such as cataract surgery.
Dry Eye After Surgery: Why Cataract Patients Often Feel It More
Dry eye syndrome is significantly influenced by aging. That point is crucial. Patients coming in for cataract surgery are more likely to already have dry eye before the operation compared with younger patients seeking vision correction surgery.

On top of that, their ability to recover from dryness triggered by surgery and by post-operative eye drops tends to be lower. That means after surgery they may experience greater discomfort related to dry eye, and artificial tears become essential rather than optional.
If artificial tears were excluded from insurance coverage, then based on current hospital rates, the patient’s out-of-pocket cost could move from about 30% to 100%—a roughly 3.3-fold increase. There has been discussion that insurance benefits for artificial tears may be maintained for elderly patients, so there is reason to hold onto hope, but in the end we have to wait and see the final outcome.
How I Decide Treatment: Severity First, Then Step-by-Step
Because causes overlap, I focus on severity and response. Many patients have symptoms without severe surface damage, and for them, the first step is often not a procedure—it’s adjusting the daily habits that silently worsen dry eye.
I typically begin by reviewing environmental and behavioral triggers. Humidifiers can help in dry indoor air, while heaters and air conditioners often worsen evaporation. I also pay close attention to intensive near tasks for long periods—smartphones, computers, and reading—because reduced blinking and sustained focus can quickly aggravate dryness. Contact lens wear is another common factor that can push borderline dryness into daily discomfort.

When we start with these basics and patients are consistent, symptoms often improve more than they expect.
Artificial Tears: The Foundation (and When They’re Not Enough)
If lifestyle changes alone aren’t sufficient, the next step is artificial tears. If artificial tears are effective, we continue them. Many patients do very well at this stage.
If they’re insufficient, I don’t just tell patients to “use more drops” and hope for the best. This is where escalation matters. We can add other medications depending on what the ocular surface needs and what type of inflammation or tear film instability is present.
I also encourage patients to learn what they’re putting in their eyes. Artificial tears became a “hot issue” recently because of price and coverage questions, but beyond cost, it’s still important to understand the ingredients and what functions they serve—especially since these are products used directly on the ocular surface, sometimes frequently, even if only for a short-term post-operative period.
Evaporative Dry Eye and Meibomian Gland Dysfunction: Warm Compresses and IPL
In older patients, dry eye is often accompanied by Meibomian gland dysfunction. In this situation, the lipid (oil) layer of the tear film is the main problem, and tears evaporate too quickly.
That is why treatment may need to go beyond standard artificial tears. I often recommend self-applied warm compresses to help improve the function of the Meibomian glands. In addition, IPL (intense pulsed light therapy) can be used to support gland function and stabilize the tear film by addressing this evaporative component.

Some patients also benefit from oral medication in selected cases, depending on their overall condition and how their symptoms behave over time.
Aqueous-Deficient Dry Eye and Sjögren’s: Keeping Tears on the Eye Longer
There are special cases where the main issue is not evaporation but insufficient production of the aqueous layer of the tear film. A well-known example is dryness associated with Sjögren’s syndrome.
In these cases, artificial tears are prescribed to supplement what the eye cannot produce adequately. But it’s not only about adding tears—it’s also about increasing the time those tears remain on the ocular surface. That is where procedures such as punctal plug insertion can be considered to slow tear drainage.
Along the same lines, high-viscosity artificial tears may be used to improve retention time, and other medications may be considered based on severity and ocular surface findings.
When Dry Eye Becomes Severe: Protecting the Cornea
If corneal epithelial damage is severe, autologous serum eye drops can also be considered. These are not “routine dry eye drops,” and severe ocular surface disease requires a higher level of care and close monitoring.
In cases that advanced, I believe it is best to refer the patient to a university hospital where the full spectrum of specialized diagnostics and treatments is available, especially when systemic disease or complex corneal damage is involved.
Conclusion: A Practical Way to Think About Dry Eye
Dry eye syndrome is defined by disruption of tear film homeostasis, but what matters to patients is the lived experience—burning, gritty discomfort, fluctuating vision, and fatigue that can affect work and quality of life. In clinic, I rarely see a single clean “cause.” I see overlapping factors, which is why I base treatment intensity on symptom severity and then move step-by-step.
For many people, starting with environment and habit changes, then using artificial tears correctly, is enough. For others—especially older patients and those with Meibomian gland dysfunction or Sjogren’s—treatment may need to include warm compresses, IPL, tear-retention strategies like punctal plugs, or more advanced therapies.
The most important message I can share is that dry eye is manageable when approached realistically and systematically. The goal is not just more drops—it’s restoring stability to the tear film and comfort to daily life.
More about Samsung Miracle Eye Clinic
Samsung Miracle Eye Clinic near Gangnam Station is a comprehensive eye center that helps patients understand the underlying causes of dry eye syndrome—such as tear film instability, meibomian gland dysfunction, screen-heavy lifestyles, contact lens wear, and post-procedure dryness—while guiding them toward practical treatment options tailored to severity, from lifestyle and lubrication strategies to targeted in-clinic care when needed. A key differentiator is its 1:1 personalized care model: each patient receives a tailored consultation and plan, and unlike many clinics, the same doctor who performs the eye exam also performs the procedure and supervises the entire recovery process for consistency and accountability. For patients combining dry-eye management with vision correction or lens-based solutions, the clinic’s One-Day System leverages an advanced in-house diagnostic pathway and patented Miracle Formula for precise lens power calculation, enabling accurate diagnosis and surgery on the same day for added convenience. The clinic is also distinguished by ambidextrous surgeons who can operate with equal precision in both eyes, supporting symmetry and accuracy while minimizing contact with the nasal bridge for comfort and safety. In addition, an experienced International Patient Team supports overseas visitors with a seamless experience across services that include SMILE LASIK, LASIK/LASEK, presbyopia-cataract treatment, intraocular lens insertion, Dream Lens (orthokeratology), and re-calibration surgery.
Find more about this clinic here: Samsung Miracle Eye Clinic