Medical Tourism Blog
Dr. Taek-Kyun Kim Q&A Rhinoplasty - The Plus
Table of contents
- Why are so many people curious about rhinoplasty in Korea?
- How do you divide the nose when planning rhinoplasty?
- What implant materials are most commonly used for rhinoplasty?
- What is the typical recovery time after rhinoplasty?
- What’s the difference between using cartilage and implants in rhinoplasty?
- Why can revision rhinoplasty be difficult?
- What should you consider when planning revision rhinoplasty?
- What are the chances of side effects when using autologous tissue?
- What is the single most important aftercare point for rhinoplasty patients?
- How should you approach your next step if you’re considering rhinoplasty?
- More about THEPLUS Plastic Surgery
Considering treatment in Korea? Everything you need to know e.g. — how to avoid scams, visas, interpreters, recovery tips — in our Medical Tourism Master Guide. Plan with confidence in minutes, not weeks!
Disclaimer: The following is a guest post. The information and opinions expressed are not of koreaclinicguide.com but of THEPLUS Plastic Surgery
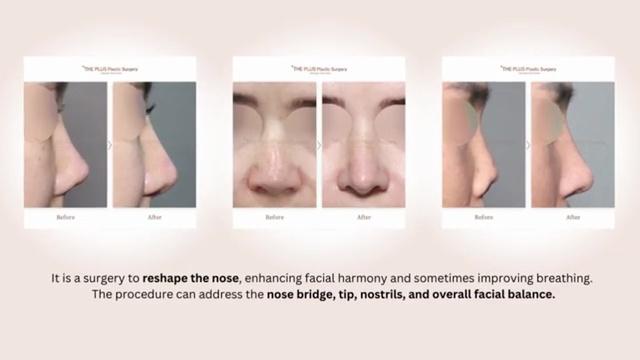
Why are so many people curious about rhinoplasty in Korea?
Rhinoplasty in Korea draws attention because patients often want a clear plan: what gets changed, what materials are used, how long swelling lasts, and what “normal life” looks like after surgery. When people come in for a consultation, I try to make the process easy to understand and practical. A nose job isn’t just about “making the nose higher” or “making the tip smaller.” It’s about choosing the right technique for the right part of the nose, using the right material in the right place, and respecting healing—because the result you love at one month should still look and feel natural years later.
How do you divide the nose when planning rhinoplasty?
For planning purposes, I like to divide the nose into four main parts: the tip, the bridge, the nasal bones, and the nostrils (the alar area). This matters because each area behaves differently and often needs a different surgical approach. The bridge is largely about structure and smooth contour. The tip is about shape, definition, and—very importantly—natural movement. The nasal bones may involve narrowing or straightening. The alar area focuses on nostril width and the overall balance of the base.
When you think about rhinoplasty this way, it becomes easier to understand why we don’t use one single material or one single method for everything.
What implant materials are most commonly used for rhinoplasty?
For the bridge, the most commonly used material is silicone, and the most common option is a silicone implant. There are other materials that can be used depending on the case and technique, but silicone is the one most people immediately think of when they hear “implant rhinoplasty.”

The important point is that material choice is not just about popularity—it’s about using the right tool for the job. The bridge needs reliable volume and stable shape. That’s why an implant is often chosen for that specific area.
What is the typical recovery time after rhinoplasty?
Recovery depends on the exact technique and which parts of the nose are operated on, but in terms of getting back to daily life, it’s usually about 1 to 2 weeks.
If it’s a simple procedure, such as working on just the tip or just the bridge, many people can plan around about one week. On the other hand, if the surgery includes an osteotomy (meaning we work on the bone) or something like an alar reduction, you should expect a bit more downtime—typically around three extra days. So overall, most patients find it helpful to think in terms of 1–2 weeks for returning to everyday routines.
What’s the difference between using cartilage and implants in rhinoplasty?
This is one of the most important concepts to understand: cartilage and implants have different roles, and they shouldn’t be treated as interchangeable.
For the tip, whether it’s ear cartilage or septal cartilage, it’s generally best to use your own tissue. The tip is not only visible—it’s also the part that should feel and move naturally. If an implant is extended all the way to the tip, the tip can lose that natural mobility and may feel hard to the touch. That’s why I typically use an implant for about two-thirds of the length of the nose, and then shape the tip mainly with ear cartilage or septal cartilage.
For the bridge, cartilage is usually not ideal as the primary volume source because there often isn’t enough of it, and it typically can’t provide the same level of structural height and smooth contour that patients want. That’s why an implant is commonly used there.
If you want the simplest way to remember it, it’s this: tip with your own tissue, bridge with an implant.
Why can revision rhinoplasty be difficult?
Revision rhinoplasty can be difficult for a few major reasons, and most of them come down to tissue quality and what happened during the first surgery (or surgeries).
One challenging situation is when there has been inflammation, and silicone had to be removed. Another is when someone had trauma, the implant was removed, they waited about six months, and then returned for another operation. In those cases, the tissue can become stiff, and the inside may be significantly damaged, making it harder to create clean, predictable changes.
Revision can also be difficult when someone has had multiple surgeries and there isn’t much usable cartilage left. In rhinoplasty, cartilage is a valuable resource, especially for tip work and for rebuilding support.
Finally, skin quality is a major factor. No matter how precisely I shape the cartilage framework underneath, what you actually see is how it appears through the skin covering it. If the skin is thick or has issues, the refined shape underneath may not show as clearly.
What should you consider when planning revision rhinoplasty?
In revision cases, I first focus on why the revision is being done. The key question is whether you want revision surgery simply to change the shape, or whether there is an actual complication.
If the revision is due to a complication, I generally believe it’s best to use autologous tissue (your own tissue) as much as possible. If it’s purely for shape, then in many cases you can use synthetic materials again.
Another important point: for the tip, I continue to favor using your own tissue, and I don’t recommend placing an implant all the way into the tip. If someone suggests extending an implant directly into the tip, I would personally be cautious and ask detailed questions about the long-term feel and movement.
And if you’ve had inflammation before, during your consultation you may want to consider a plan that leans more toward autologous tissue.
What are the chances of side effects when using autologous tissue?
With autologous tissue, infection is extremely rare, but that doesn’t mean problems are impossible. A graft has to settle in and survive, and for that it needs adequate blood supply and nutrients.
This is where lifestyle matters—especially smoking. If someone smokes around the time of surgery, the graft may not receive what it needs to integrate properly. In that situation, it may not be a classic infection at first; it can be graft failure. But once tissue struggles inside and continues to cause issues, it can eventually lead to a secondary infection later on.
So while infection with autologous tissue is uncommon, the overall outcome still depends heavily on good healing conditions.
What is the single most important aftercare point for rhinoplasty patients?
If I had to choose one message to repeat, it would be this: absolutely no smoking around the time of surgery. I emphasize it again and again because it’s truly that important. Surgery technique matters, but patient aftercare can protect—or undermine—the result.
Good healing is not only about looking less swollen sooner. It’s about the long-term stability of the structures we build and the health of the tissue that needs to recover.
How should you approach your next step if you’re considering rhinoplasty?
If you’re thinking about rhinoplasty in Korea, I recommend approaching it with a simple framework: understand which part of the nose you want to improve (tip, bridge, bones, or alar area), then match the method and materials to that goal. In many cases, a natural-feeling result comes from respecting each material’s role—cartilage for the tip, implant support for the bridge—and planning realistic recovery time based on whether bone work or alar reduction is involved.
When you’re ready, the best next step is a thorough consultation where we can talk through your anatomy, your goals, and the safest way to achieve a balanced, natural outcome.
More about THEPLUS Plastic Surgery
THE PLUS Plastic Surgery, located in Garosu-gil, Gangnam, Seoul, is known in Korea for rhinoplasty and revision rhinoplasty backed by a research-driven, education-leading team and a start-to-finish system that spans consultation, surgery, and post-operative skincare across four dedicated floors. The clinic is led by two highly regarded rhinoplasty authorities: Dr. Kim Taek Kyun, a board-certified plastic surgeon recognized internationally for award-winning research on 3D implants and for running annual training sessions for fellow surgeons, and Dr. Jeong Jae Yong, President of the Korean Society of Plastic Surgeons, who is frequently invited to speak on rhinoplasty—especially revision cases—at major global forums and emphasizes outcomes that unite function (breathing and structure) with beauty. In terms of materials, THE PLUS tailors the plan to facial harmony and patient anatomy, offering both implant rhinoplasty options (informed by advanced implant research and precise design) and non-implant approaches using the patient’s own tissue when appropriate, with careful selection aimed at natural-looking, stable support. For recovery in Korea, patients commonly experience the most noticeable swelling and congestion in the first 72 hours, with bruising and swelling gradually improving over the first week; splints and any external sutures are often addressed around days 5–7 depending on the technique, many people look more socially presentable by 1–2 weeks, and the nose continues refining as residual swelling settles over 1–3 months, with definition and final contour typically maturing over 6–12 months (timing varies by procedure type, revision complexity, and individual healing).
Find more about this clinic here: THEPLUS Plastic Surgery















